
She already had surgery for "elbow tendinitis" (radial nerve release) and that had returned after a while. Here is here evaluation.
Subjective: Pt reports insidious onset of B wrist pain at least 1 year ago or more, most likely from repetitive motion. Sx are felt in anterior wrist radiating into thumbs. She is right handed but felt L > R, since onset Sx have been worsening. Sx are constant and rated 7-9/10. Sx worse in the morning, with wrist flexion, driving, grasping. Sx better when wearing braces.
Objective: fair sitting posture, moderate forward head
key: F = functional (WNL), D = dysfunctional, N = non-painful, P = painful, PDM = pain during movement, ERP = end range pain, LRF = lat rotation and flexion, MRE = med rotation and extension
ROM
Cervical
flexion FN
extension FN
Rot/flex Left DN, mod Right DN, mod
Shoulder
LRF Left FN Right FN
MRE Left FN Right DN, mod
Forearm
Supination Left DN, mild Right DN, mild
Pronation Left FN Right FN
Wrist
Flexion Left FN Right FN
Extension Left DN, mod Right DN, mod
Myofascia: moderate restrictions along median and radial upper and lower patterns, L > R cervical paraspinals, upper traps
Special tests: upper limb neurodynamic test mod limited bilaterally with median, radial nerve bias. Corrected sitting posture decreases wrist complaints and paraesthesia with wrist movement.
So here is the thing about her postural correction test, ala MDT cause and effect. Initial postural correction did not change the pain in her hands/wrists. However, prior to it, she stated increased paraesthesia with light wrist flexion/extension. I asked her to try this again while I held her in cervical retraction and scapula set position. To her surprise, the paraesthesia was gone!
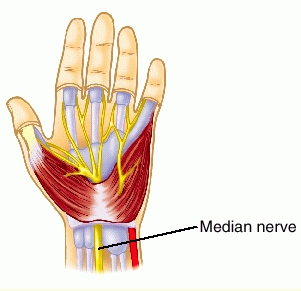
Treatment 1: IASTM to the radial and medial nerve containers first left and then right. As a pre-test, I took median neurodynamic measurement on the left, it was mod to sev restricted with pain and difficulty with elbow extension past 70 degrees bilaterally. After IASTM on the left, she stated there was a significant relief to the pain in her left wrist and hand. Median neurodynamics had only minor wrist extension limits and was barely uncomfortable according to the patient.
Prior to starting treatment on the right, I went for another baseline (previously being just as limited on the left), to both of our surprises, the right had improved just as much as the left! This was an amazing neurophysiologic effect! I expected some improvement, but not like I had already done the entire treatment! I still did the IASTM and finished with some light IASTM to the cervical paraspinals and upper traps.
She was instructed on the use of a lumbar roll at work (she is a NYS Thruway toll operator) and on the median nerve prayer tensioner for HEP
Treatment 2-3: She reported feeling at least 85% better with main complaints only being in her left thumb. Most of her ADLs are no longer limited, but she is still wearing her braces at night. I added subcranial inhibitive distraction technique for the upper cervical area. I also added light IASTM to her thenar eminence and posterior aspect of the bony contours of her first metacarpal on the left.
Treatment 4: There is still no change to her left thumb, I performed treatment as above, and changed the HEP to another median neurodynamic tensioner; this one is similar to pushing against a wall, but with emphasis on finger opening and closing, especially her first three digits. This was the last time I saw her, so there is more to come!










Post a Comment
Post a Comment