
Indications for this technique are:
- restrictions in subcranial/OA forward bending, bilaterally or unilaterally
- unilateral or bilateral HA that are improved, but possibly plateaued from previous techniques
- TRANSVERSE LIGAMENT LAXITY
WHAT???? This technique, developed originally by Dr. Stanley Paris, was for those with subcranial dysfunction, but after trauma or otherwise, had laxity which fell into the hypermobile category, but not instability. Normally, bilateral techniques such as OA Rock, Subcranial Distraction with or without shear would be contraindicated. Since this is a unilateral technique, it does not stress the transverse ligament of the atlas.
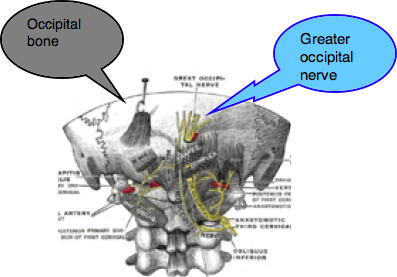
When blocking the lateral posterior portion of the atlas, make sure you push P/A and take up the tissue slack. The patient may complain of severe tenderness and possible referral to the eye/orbits. This is why it is nicknamed, "The Hot Poker." Once you're on the atlas and properly stabilizing it with your second and third digit fingertips, you nod the patient passively, actively, or active assistively in that direction as demonstrated in the video. Two to three reps sufficient per side if you are performing it bilaterally with as many sets per treatment day. Note, this also acts as a PIVM test since you can grade accessory motion with it. I usually perform this after 5-10 minutes of TASTM or STM to the area. Cervical retraction or OA nodding with slight rotation to the side of the treatment work as a HEP 10 reps hourly. Watch the video for a better explanation of the technique. Comment or question below! I hope you find this helpful with your patients!











