

I wonder if head-bangers report less pain and dysfunction after an MVI?
W.A.D.
Whiplash, known to practitioners as “WAD” or Whiplash Associative Disorder, is a collection of symptoms associated with a specific traumatic onset. If you are familiar with rehabbing this cohort, you’ll know that symptoms tend to be more chronic in nature, and it is a condition that tends to respond differently than the typical mechanical neck pain patient.
This blog will discuss some thoughts toward WAD diagnosis, its’ unique attributes and potential rehab strategies.
A MUCH NOVEL STIMULUS:
The first factor of whiplash to mention might be its uniqueness: it’s the opposite of an insidious onset, and puts the body (the cervical spine in particular) through a particular load at a particular speed that it is likely very unfamiliar with. Taking all other factors out of the injury (the emotional trauma of being hit by another vehicle) this rapid change in tissue homeostasis and change in mechanical load and tensile forces detected as afferent input is impossible for the brain to ignore. There are all sorts of tissues being stressed: facet, ligaments, soft tissues and all their inherent sensory innervation. Mechanoreceptors responsible for communicating muscle tendon tensile status to the brain, are registering something off the charts.
Why is this situation, the sensory innervation being bombarded with new information, particularly conducive to a pain state? Part of the answer is context, part is that this how our bodies are designed to respond.
TRIGGERED RESPONSE:
When our tissues undergo abnormal stresses and strains, regardless of insult to tissue integrity or physiological changes in the tissues from these forces, our body (via our brain) “lets us know” and becomes temporarily sensitized (after that is, ensuring that we are going to survive). This sensitization is especially in tune with not only the specific way the tissues were stressed, but also the environment they were stressed in. This is where the analogy of a sunburn can be of use: the day after a sunburn, what does being in the sun feel like? Is that sun any different than the day before? No, but it sure feels different. Its your bodies way of telling you it experienced more than average of some stimulus, and it is going to create a scenario where you can now monitor this, and be aware of this. Without going into the minute intricacies of sensitization, the basic concept is that the tissues that underwent the most stress are going to then register similar stresses with heightened awareness, and as potentially threatening. This will continue until the tissues return to normal homeostasis, or adapt to a new level of stress.
“The evidence suggests that pain mechanisms can move or shift as time goes on and the relevance of the tissue lesion diminishes in an inversely proportional way to the relevance of chances in the central nervous system” – Louis Gifford, on WAD (7)
THE CONTEXT:
This is particularly relevant to WAD. You can have a “Triggered Response” that is highly variable depending on the context of that response. The reason patients seeking medical attention for WAD is ubiquitous and often difficult to treat is the context of the injury. Whiplash is accompanied by an inherently threatening situation (unlike most insidious pains) and often this situation can be blamed on someone else. Now you have a situation where the normal responses of pain, tightness, headache etc are under constant interpretation of blame: “If it weren’t for that (insert your profanity here) I wouldn’t be feeling like this, look at all the difficulties I’m having with even mundane activity- all of this is because of that accident and that idiot driver”. All the symptoms are real, and initially true tissue damage is often present, but propagated by this reaction. If it seems hard to grasp that concept, think of how our current state of thought reflects in what we feel in our bodies. When we are stressed, anxious, depressed, it is easy to notice some changes in how our body feels. Especially that whiplash is often sustained by an increase in tone, thinking recurrent thoughts of frustration and blame just ramp up the current condition.
This brings to mind an experience I had a month ago with some late season snowboarding. I was slammed pretty hard after a failed attempt at a spin of a small feature, landing 90 degrees shy of where I wanted and catching a backside edge: which is always followed by sort of a body slam to the back motion and the head follows.

Shot from the GoPro at Keystone…
I rode the rest of the day, without too much worry to it. The next morning my neck had about 50% of its normal range, super sore, super sensitive. I couldn’t lift my head directly from a pillow for about a week- I needed to assist a little with my hand and then I was good. I kept busy at work and tried not to think on it much. I was more amused by it than anything: I knew it would go away, I’d had this before, and I could almost approach it with a sense of curiosity instead of impending doom. This could be a key factor in a normal recovery and good outcome. I realize my mini-whiplash was probably much less intense than many WAD patient incur, but there are some useful principals in management there. I am sure, that if the exact same stresses had have occurred, but as result of some car not paying attention to what they were doing and slamming my car, I my pain would have responded differently. I might be better and trying to meta-cognate on the influences of pain, but I wouldn’t be surprised if the recovery was 2-3x longer, and accompanied resentment toward the driver (why do I have to work all day with stiffness and pain because you weren’t paying attention??). Instead, I took complete onus for the event, thus I was really just waiting for tissues to undergo their proper physiological process after the high stress event, and viewed the symptoms as expected temporary changes.
I’ve actually tried a tactic (verdicts still out whether its appropriate) with WAD patients, at the appropriate time (emotions subside and they are showing signs of grasping the situation and confidence) instructing them to “if you are willing, really try to reinterpret your pain for the next 4 weeks and act as if the pain you have now was from a fall you had last time you went skiing (or whatever activity they are into- maybe head-banging at a concert) If the idea seems silly then we will find lots of other ways to help get over this..”. The downside is appearing insensitive, but I think if you could reinterpret the pain and separate it from incident, this would help.
THE IMPLICATIONS:
The fact that the same “injury” or stress can fall upon tissue and that tissue react in vastly different ways is evidence that we are not after a specific tissue impairment here with these WAD patients. Moreover, we are seeking to be a catalyst in returning tissue to its normal state (unless there is reason to suspect true tissue failure, such as transverse ligament of the atlas rupture or odontoid fracture). Even if there were “findings” of (enter manual assessment here) these findings are a response to injury, and a reflection of the CNS sensitivity. Applying techniques to reverse these are usually futile in a sensitive state: poking the bear can have its place in terms of looking for adaptations and desensitization, but with this cohort any poking needs to come from an internal locust of control buy having the patient work on being able to test their own limits with constant monitor of their response (this could be through simple exercise), as they have all ready had enough “outside influenced stimulus” as evident in their MOI.
THE DAMAGE
We must first note the often tenuous link between what we view as “damage” and whether or not that is influencing the pain. We just don’t have a clear view of this. Some of it may be from lack of sensitivity of imaging, and much is from lack of true relation. However, damage aside, inflammatory responses can be viewed as somewhat causative. It may be better to look at tissues response (whether muscle, ligament, disc or facet) rather than its actual state (facet arthropathy, annular tear, disc bulge).
There is surely potential for damaged tissue post the stresses induced by whiplash. However, seeking to locate the damaged tissue and affect it manually by simply applying inputs may prove futile. Tissues heal at vary different rates due to their blood supply (so disc and ligament may be delivering their inputs to the brain for a long time post injury, thus creating a scenario more conducive to pain, with prolonged chemical or metabolic activity happening at the site of the lesion) and it is further difficult to pinpoint specific tissues with specific tests. Further, think about the relation between tissue abnormalities and pain- it is certainly not always a clear link.
“While evidence from in vitro studies indicates that the injury can damage any number of anatomical structures in the cervical spine at any segmental level, it is largely unknown if these lesions occur either in combination or are independent of one another. However, one thing remains clear: whiplash injury can, in some patients, trigger a cascade of events that promotes the development of chronic symptoms. It is, therefore, crucial that emphasis be directed towards understanding the underlying mechanisms and subsequent sequelae of the condition” -Jim Elliot (1)
THE REHAB
We can’t think along the lines of “fixing the (facet, disc, or muscle)” or have the patient be under the impression that this is the absolute pathway to recovery. We also can’t think along the lines of “just let it heal” either, because the seemingly culprit lesion may only be relevant in initial stages of trauma, and the chronicity of pain driven by maladaptive changes in processing. And there isn’t one access point to these maladaptive changes: its multi-factorial. This means striving to consider how the patient thinks about their condition, their beliefs of injury, their additional stressors (litigation, job stress, road anxiety), their movement habits (the list goes on) have impact on the current disability, and how these areas might me modified or re-conceptualized.
"Emerging evidence suggests that clinical focus should be directed towards treatment schemas that better address identified dysfunction and clinical examination findings that have been shown to characterize the acute and chronic conditions (eg, alterations in the sensory and motor systems, and signs and symptoms of psychological distress)." -Elliot (1)
All pains are multi-dimensional, and “biopsychosocial”, however WAD pain is an especially “3D” pain due to its context:
- Sensory Dimension: (afferent inputs, perception of pain and where it is, its’ behaviors and “attitudes”) *where most practitioners focus
- Cognitive Dimension: How we process what we are feeling, our beliefs, essentially how our thoughts affect our pain; “this person did this to me”, “I have a disc degeneration”, “my spine is messed up”...
- Emotional Dimension: with pain come emotional reaction: how our behavior changes, how we approach our environment in reflection of our pain.
"Pain is a biopsychosocial experience that goes well beyond mere nociception. In this regard, identification of the physical pathology at the site of injury is necessary but not sufficient to explicate the complex process by which somatosensory information is transformed into the physiological, cognitive, affective, and behavioral response labeled as pain" - Garland (2)
What is a WAD patient working with?
- High stress and anxiety, usually a "sympathetic dominated state"
- Possibly centrally mediated somatosensory alteration (1)
- Widespread sensory hypersensitivity (or decreased pain thresholds) (1)
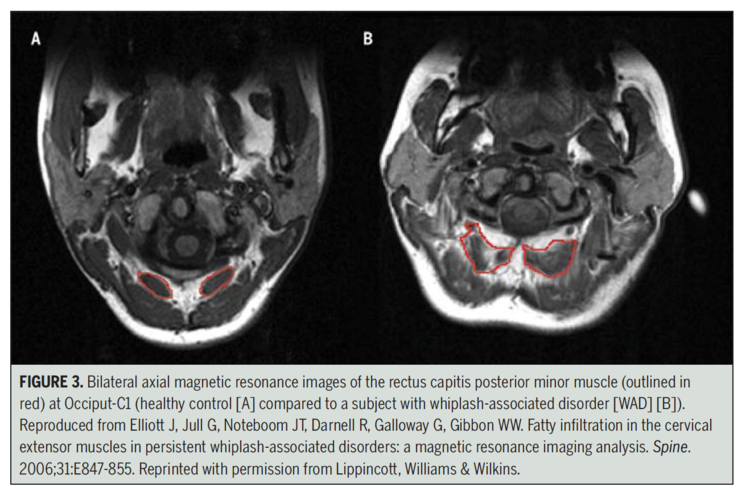
- Presence of muscular degeneration (fatty infiltration) in the cervical extensor muscles (1)
- Dizziness and disturbances to the postural control system (5)
- Impaired neuromotor control, detected in the CCFT (crainio-cervical flexion test) (4)
- Reduced standing balance and increased sway (1)
- Reduced cervical ROM (especially in rotation) (6)
- Possible oculomotor dysfunction (3)
- Jerky movement, not your normal smooth motions (altered motor strategy and co-contraction)
There is no recipe or protocol for WAD patients. We can apply what we know about sensitivity, how tissue reacts, concepts of graded exposure and relaxation, and patient assurance in seeking a good outcome.
I think the initial visit needs to be met with highlighting some of the above commentary: there is no “quick fix” but this doesn’t entail that something is broken. Tissue damage can definitely exist in the acute stage, but the patient should be taught to view their tissues as de-conditioned as opposed to damaged. This will allow them to have more confidence in their rehab. They also need to tune in to emotional influence. It is often pretty transparent to the patient that their emotional response is affecting their pain: they often claim that driving is very difficult and accompanied by lots of pain, stress and tension. I have had a few patients that I have instructed to just go sit in their car for 10 minutes, a few times per day (these were the patients that would break down to tears when even talking of the incident, and refused to get behind the wheel). This is an example of graded exposure: first sitting in the car, then driving around the block, then ramping up from there. These tactics are not directly aimed at the tissue obviously, but indirectly affect the tissue through how the body responds to situations, with the hope of less response over time.
To assist in reducing tone and prompting a more "parasympathetic" state, diaphragm breathing is always taught with this cohort. The relationship between sensitized state and sympathetic nervous system activity, and its counterparts can be explained if desired.
As with any rehab program, movement and strength are going to be important, and trying to find the balance in how much you can push these elements will be based on patient response.
- High sensitization: patient education, belly breathing, very light self assisted cervical isometrics, small ROM exercises based on trying to “relax and move” such as fluid figure 8 movements in a small range and progressing from there, working on “indirect rotation and movements” from the bottom up, walking and introducing exercise distal to the sensitive tissue (cycle etc). Educate on the fact that their tissue response is normal, and that not moving or rest is actually more detrimental. Exercise may be used distally (like cycling) for psychological benefits as well as vascular benefit. The risk of manual therapy does not out-weight the benefit in this group.
- Low sensitization: same as above but working on increasing intensity as tolerance allows. Deep neck flexor exercises, prolonged isometrics, upper body exercise, and hopefully a program of return to activity they enjoy that is graded in intensity.
The “strength” exercise may be supplemented with education that “were trying to get the muscles to start acting normal again and responding how they should to work (not explained as your core neck muscles are very weak and can’t support your head). Patients may have overactive superficial muscles and weaker deep muscles as Jull notes with the CCFT performance in a WAD cohort.

The Cranio-Cervical Flexion Tests: Jull et al.
As noted, muscle tissue makeup also undergoes changes. These areas which gain fat infiltration are known for their proprioceptive density, which could explain some of the loss of motor control and balance that accompanies WAD. This finding was also specific to WAD population (and not in chronic neck pain population) thus it is likely not only from disuse. Inflammatory processes may be more culprit in this finding in WAD patients, and WAD patients also differ in sensory and psychological measures (what I interpret to mean is that WAD patients tend have an overall more central sensitized state and remain so…)
Decreased range of motion may reflect underlying disturbances in motor function as a consequence of the initial peripheral nociceptive input resulting from injured anatomical cervical structures. (1)
The muscles are inhibited or using abnormal strategy, and sensitive to work because it is a form of stress. It is safe stress, but the body doesn’t always decipher that, so we can always find a starting point and slowly build up. Prolonged bed rest is only going to push back this starting point, as we need these tissues to be experiencing things, and we expect this to initially be a bit difficult and sore.
We need to also contemplate whether/how much the patients’ beliefs and attitudes are holding them in a state of altered motor-control, increased stress, tissue hypoxia, and overall maladaptive way.
“Recent evidence suggests that disturbances to the postural control system are more likely to underlie these symptoms due to traumatic damage to the vestibular receptors, neck receptors, or directly to the central nervous system. Dizziness of cervical origin has been defined as a non-specific sensation of altered orientation in space and dysequilibrium. It originates from abnormal afferent activity from the extensive neck muscle and joint proprioceptors, which converges in the central nervous system with vestibular and visual signals, confusing the postural control system” -Treleaven (5)
WAD patients demonstrate altered “Joint Positional Awareness”, meaning that they are not as good at telling where their head is in space. The research noting fatty infiltration in some of the proprioceptive dense tissues in the suboccipitals, which could account for some of this deficit, as well as general balance and motor control deficit. You can both assess and train positional awareness with a simple laser pointer and target. You can also work on motor skill, by slowly tracking patterns on the wall with a laser, at various speeds clockwise and counter clockwise. WAD Patients also have larger loss of ROM, particularly in rotation (possibly due to hypertonic or unwilling AA rotation via suboccipital tone?) though efforts to re-gain this in a non-threatening way and re-train this with motor control may be of value.
As we have seen in other areas of the body, even after patients become pain free, they still show deficits in positional awareness and muscle endurance, which could (possibly) set a stage for recurring injury. Below are some examples of exercise, that can be an adjunct to your typical program of graded exposure towards ROM and strength and addressing cognitive and emotional influences of pain.
SOME EXAMPLES OF EXERCISES USING VISUAL FEEDBACK:
Below are some examples of potential exercises: you could also do without visual feedback (the visual feedback just allows an external focus and makes motor control and strategy visible to both patient and practitioner. I find it sometimes helpful to use because it directs attention away from neck movement per say, and more towards the goal of making the laser move, which is accompanied by neck movement). "Indirect rotation" techniques allow the tissues to undergo stresses into new ranges in a different context (perhaps less threatening) and can allow the patient to realize the canmove (show them after the exercise, "see you just rotated your neck fully with very little pain")- this might be encouraging. The "motor control" components are attempted to re-establish fine motor skill with constant scrutiny to accuracy from the visual feedback. This can be applied in various positions (neutral standing, seated, in rotation standing, or seated, standing on one leg, combine with a verbal or other body task etc...). Further, simple balance exercise may be warranted to allow the patient to practice postural control mechanisms globally.
Here are a few video examples:
SET REALISTIC EXPECTATIONS
Explain that abolishment of pain after WAD is typically slow, for reasons mentioned above. Explain that it is very common to have a roller coaster like pain, where one day it will flare up for no reason. Explain flare-ups as protective behavior, and the body acclimating to the demands of life again. If there is rapid progress, great! If it is slow, than that is normal. We can’t force a tissue state to change and need to respect that, but we can attempt to effect all things influencing it.
 -Tal Blair, DPT
-Tal Blair, DPT







Post a Comment
Post a Comment