

Dr. E here, today's guest post is from Dr. Jake McCrowell, a frequent contributor to my Physio Answers blog. Thanks to Jake for this great post, looking at what research states about some of our more common manual interventions.
Several skilled clinicians stress the importance of getting a ‘Reset’ or performing an intervention that improves mobility or motor control prior to retraining. So what exactly is a Reset? A Reset is an intervention that will heighten sensory awareness so that the patient moves and feels better (quantity, quality, or both). Several studies have demonstrated that Resets like manipulations or trigger point dry needling can improve mobility, or the quantity of movement (I'm not going to hit on this now). But are we sure that were actually getting a true Reset without other neuro-physiological changes happening? what about Resets for motor control/stability issues?
I wanted to point out some research that conveys how Resets get better movement from a qualitative standpoint. In other words, how do Resets get people moving better from a physiological and pain perception standpoint. I’ll hit on 3 major Resets: Spinal Manipulation, Trigger Point Dry needling (TDN), and Repeated End Range Loading (MDT).
1. Spinal Manipulation Reset:
The Journal of Orthopaedic & Sports Physical Therapy will be publishing an article (Thats right, I'm writing about articles before they are released!) that looks at the effects of spinal manipulation on the levels of anti-nociceptive chemicals like neurotensin (which modulates a dopamine response) and cortisol (used to activate anti-stress and anti-inflammatory pathways).
The research found increased concentration of these pain reducing chemicals immediately after a manipulation compared to the control (non-manipulation group). So what's this mean? Following a manipulation, we’re seeing a biomechanical change (quantity) and a chemical change that is likely produced as to allow for tissue deformation. The manipulation tells the joint and dysfunctional pattern to perceive less pain so that an improvement in movement quality may be allowed. In addition, the research demonstrated that the manipulation did not have long term effects of anti-nociceptive chemicals thus reaffirming the importance of combining exercise interventions and reloading the new tissue after a Reset.
2. TDN Reset:
Active trigger points (ATrP) are associated with pain, are very tender to palpation (allodynia), and contribute to multiple motor dysfunctions including improper muscle activation and restricted ROM. Muscle pain is often caused by the peripheral sensitization, or over facilitation of local muscle nociceptors. Meaning, when muscles are hurt they release chemicals to help with healing (inflammatory mediators) and to protect them (pain mediators). “Nociceptive terminals in muscle have a multitude of different receptors in their membranes, including matched receptors for molecules that are released from damaged tissue such as bradykinin, serotonin, protons (H+), and prostaglandins.” The continued presence of these inflammatory and pain mediators may be the cause for persistent muscle pain. The following research has documented these differences between that of normal muscle and muscle with painful TrPs in regards to the above chemical mediators. In it, they found concentrations for all pain and inflammatory chemicals were higher in active TrP subjects than in normal subjects as well as pH was lower (more acidic). “Subjects with active MTPs in the trapezius muscle have a biochemical milieu of selected inflammatory mediators, neuropeptides, cytokines, and catecholamines different from subjects with latent or absent MTPs in their trapezius.”
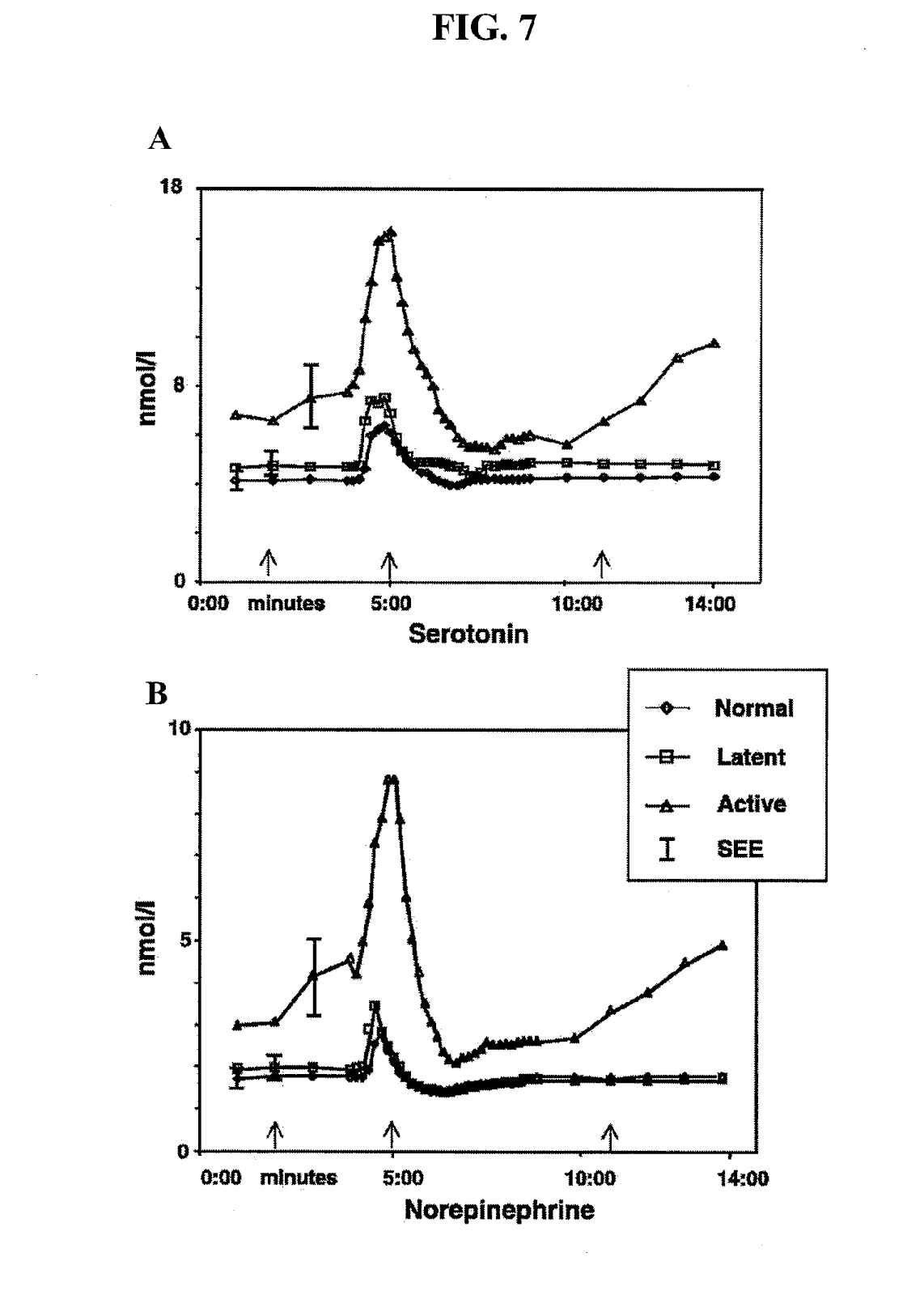
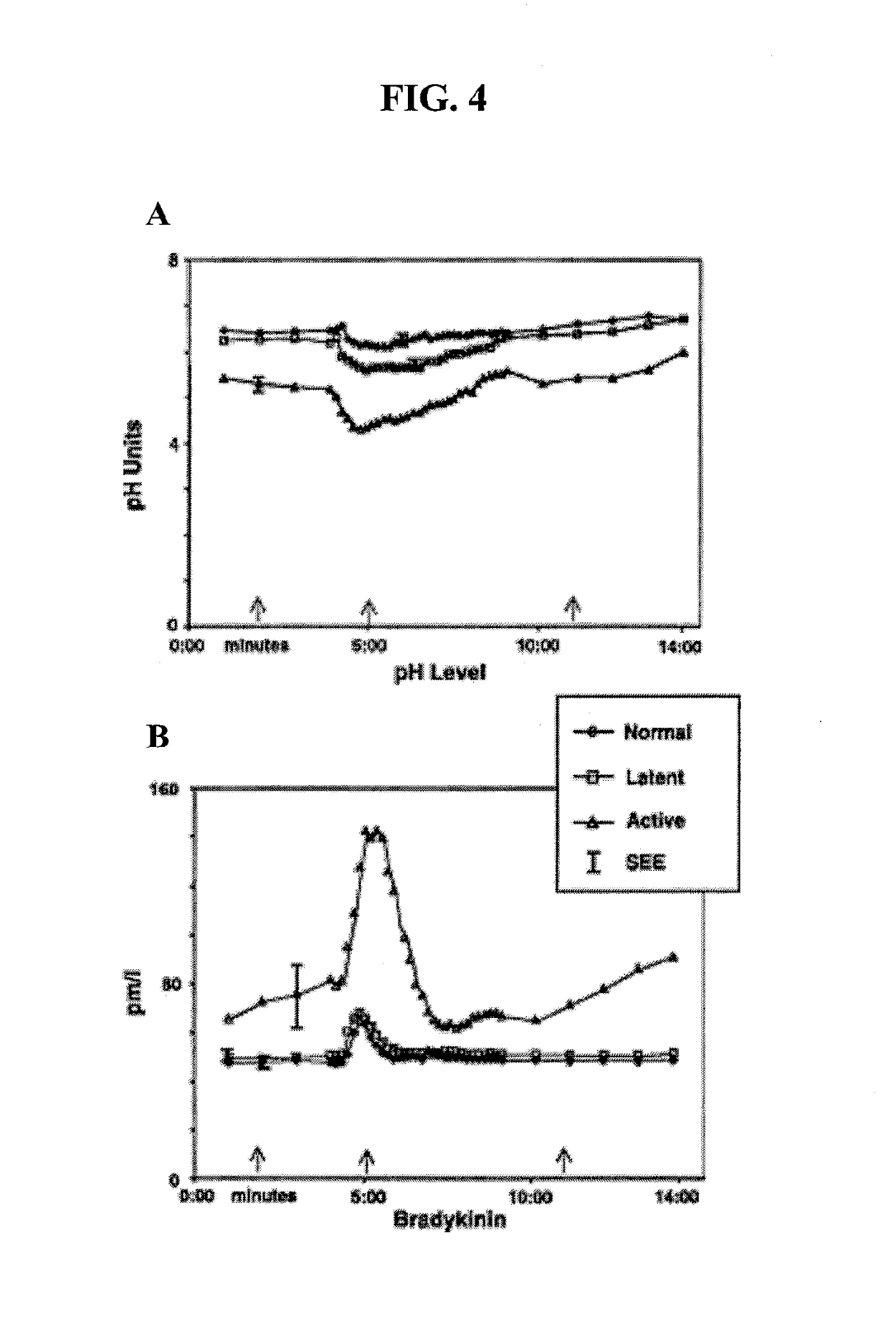
Therefore, the goal of TDN Resets of the active TrP is to elicit multiple LTRs so to alter these chemical mediators. In the active TrP group, pain and chemical mediators after the LTR (post) were significantly below their concentrations at baseline (pre). “This corresponds with the commonly observed decrease (at least temporarily) in pain and local tenderness after the release of an TrP by needling. Physiologically, this may be caused by interference with nociceptor membrane channels or transport mechanisms associated with a briefly augmented inflammatory response. The levels of these analytes may also fall because of a local increase in blood flow.” TDN Resets multi-factorially improve muscle quality, thereby providing a better base to build sound movement.
3. MDT Resets:
This one is a little less straightforward because to mine and other’s knowledge there is no specific study that looks at the biochemical effects of repeated end-range movements. We say at end range is “where the magic happens;” however it would be nice to see research to show some chemical changes correlated to this “magic.” That being said, repeated end range is a fabulous Reset technique I often use with amazing in-visit results. 
Powers et al in a 2008 study found the same improvements with repeated extensions in lying when compared to spinal mobilization (a known reset) in both pain modulation and range (spinal extension) of motion. Ensuring repeated end range can have the same mechanical and physiological improvements as other reset techniques. “Passive motion has been reported to selectively stretch contracted tissues without damaging healthy adjacent tissues In addition, repetitive movements are thought to distribute synovial fluid over the articular cartilage and disk, resulting in less resistance to motion. With less resistance to motion, subjects may have felt free to move and thus may have experienced less pain.”
“In addition to the mechanical explanation as to how repeated exercise may influence pain and motion, recent studies have suggested a neurophysiological explanation. For example, dorsal horn activation from a painful stimulus has been shown to decrease following joint mobilization.” This could explain the findings that passive movements applied to the spine elevated pain thresholds to various mechanical stimuli. In addition, if the motion produced by the press-up maneuver during the pre-treatment MRI assessment was limited by protective muscle guarding, then a reduction in alpha motor neuron excitability may have decreased the guarding response and thus allowed more movement during the post-treatment MRI assessment.
There you have it, Resets do give you a neurophysical change that assist with the biomechanical improvements that lead to improved ROM and enhanced motor control.
Thanks again to Dr. Jake McCrowell for this great contribution to The Manual Therapist. His website is Direct Performance Physical Therapy, make sure to follow it regularly for more great posts like this one!










{kind=link}
Post a Comment
Post a Comment